
Cutting Through the Noise: Understanding the Measles Outbreak and Debunking Vaccine Myths

In our current media environment with a daily onslaught of information from every angle, it’s harder than ever to separate fact from fiction. Sensationalized headlines. Fear-driven narratives. Dis/Misinformation campaigns. Some stories get blown out of proportion, while others struggle to break through the noise.
One public health crisis facing all these challenges right now? The ongoing measles outbreak in the US.
Despite being a vaccine-preventable disease, measles is making a dangerous comeback in the last decade, fueled by declining vaccination rates and rampant misinformation. But this current outbreak isn’t unprecedented. And we have the tools to get it under control.
Current status of the outbreak in the US
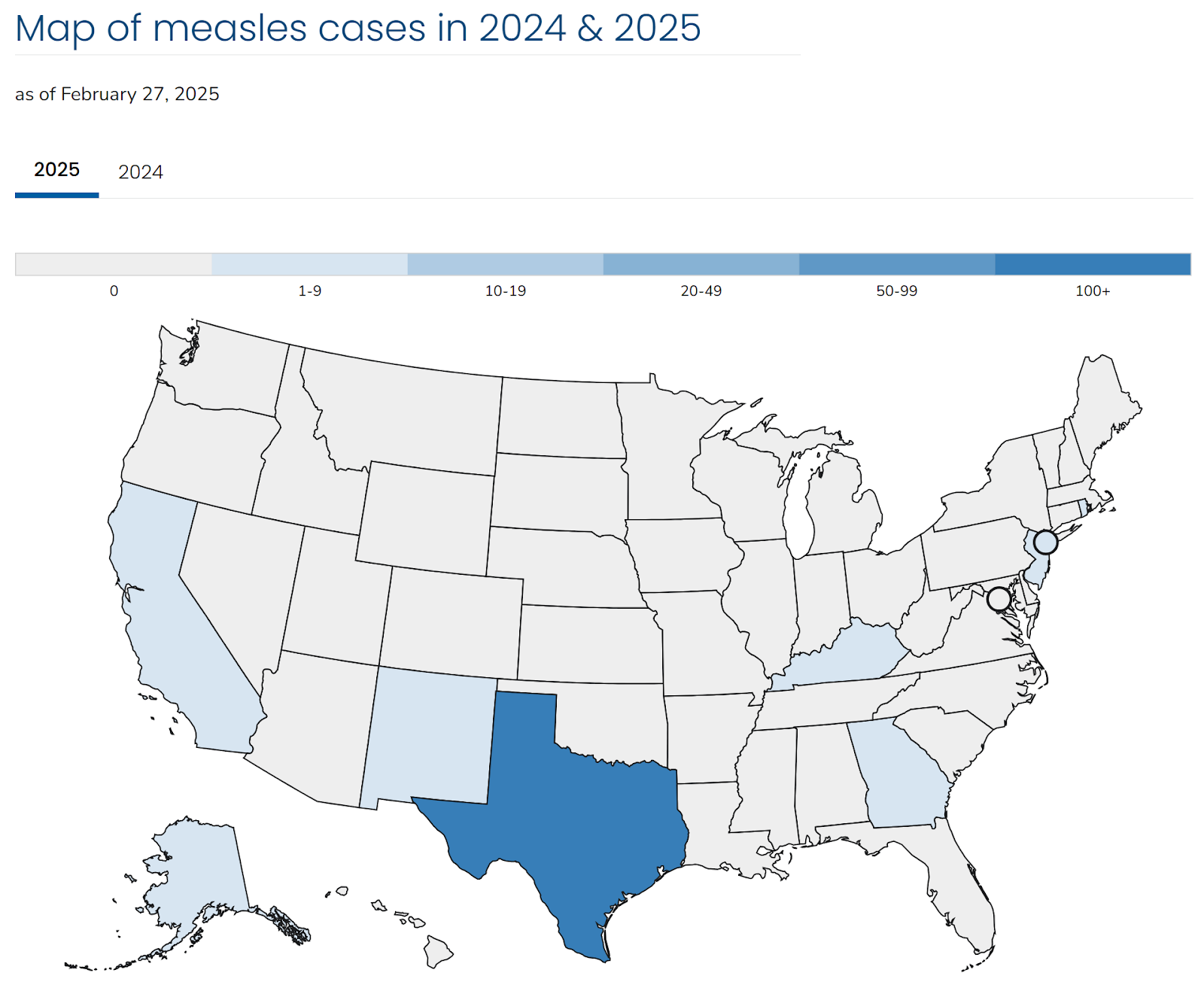
As of Feb 28th, the Texas Department of State Health Services has reported 146 confirmed cases, with 20 hospitalizations and one death of a school-aged child who was unvaccinated.
Among the 146 cases, 95% were unvaccinated; 3% had received one MMR dose, and 2% were fully vaccinated with two MMR doses. Roughly half were 5-19 years old, and another third under 5 years old.
Cases have also been reported across other states, including New Mexico, Alaska, California, Georgia, New Jersey, New York City, and Rhode Island.
How low vaccination rates fuel measles outbreaks
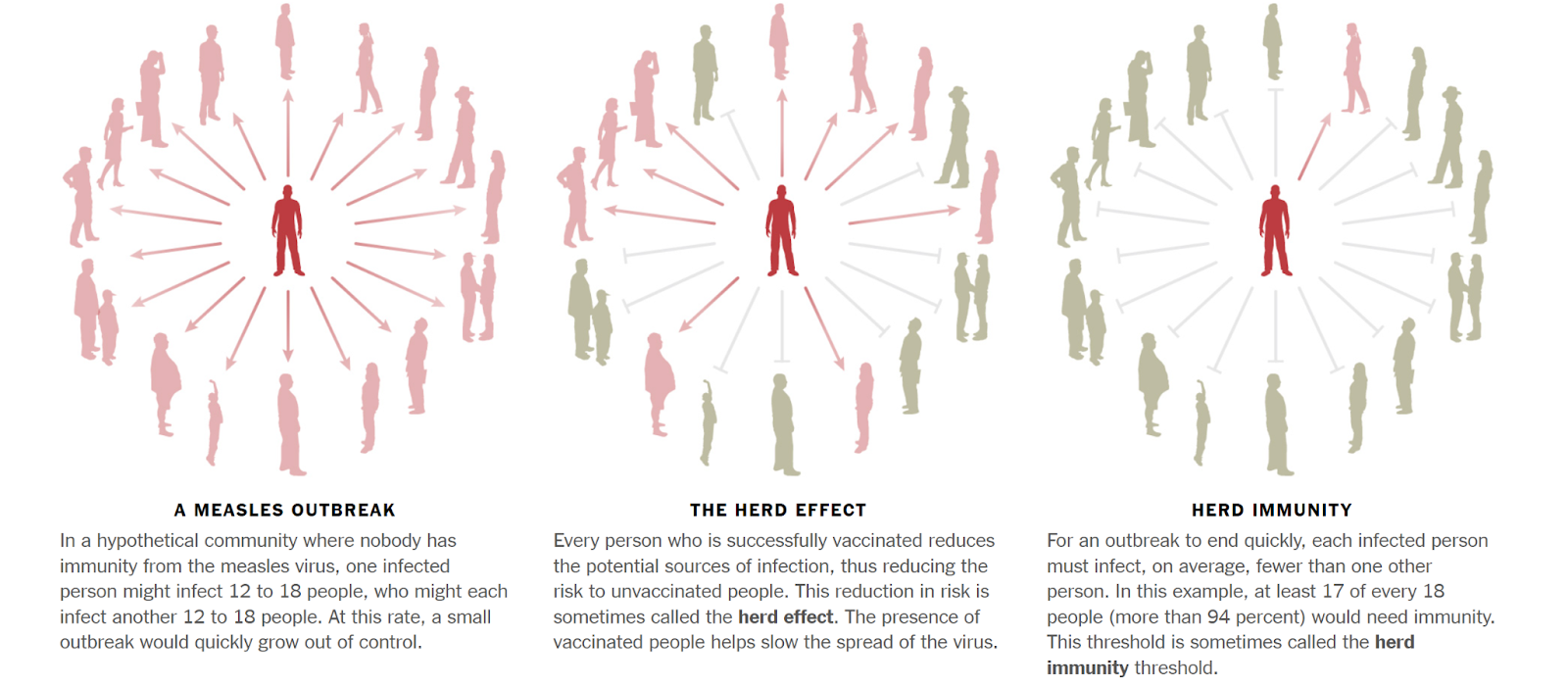
The vaccination rate within a community necessary to achieve herd immunity for measles is >95%. Herd immunity means enough individuals in a population are immune to a disease (most often via vaccination) that it becomes difficult for the pathogen to spread human-to-human among those susceptible.
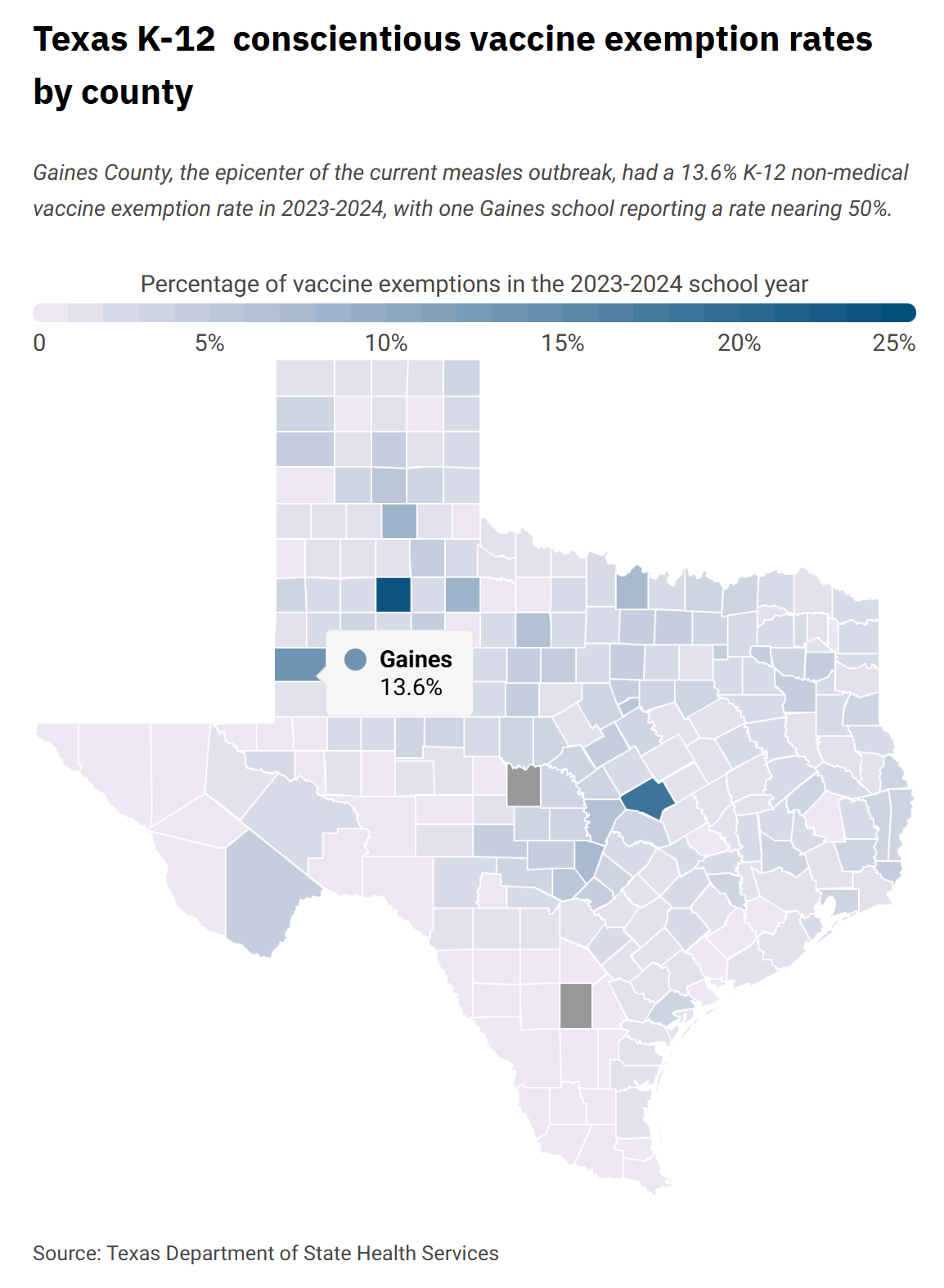
Gaines County, Texas, ground zero for the current measles outbreak, has a markedly low vaccination rate of 82%. One private Montessori school reportedly had a vaccination rate of 40% of kindergartners during the 2023-24 school year. Texas state law allows vaccine exemptions in three cases: a healthcare provider determines it’s not safe for a student to get a certain vaccine, the student is in the US military, or the student has a religious or personal belief that goes against getting immunized (ie, conscientious exemption).
Precedent: How the 2025 measles outbreak compares to previous outbreaks
A vaccine against measles first became available in the US in 1963. Due to widespread vaccination efforts and improved control, measles was declared ELIMINATED in the US in 2000. This means that while measles cases could still occur (often due to international travel), there was no sustained transmission of the virus in the US for a full year.
Unfortunately, thanks to the modern anti-vaccine movement, declining vaccination rates have led to a resurgence. (This isn’t the first anti-vax uprising, the Anti-Vaccination Society of America was founded in 1879, but this privileged ideology is critically impacting many communicable diseases across the globe.) The current outbreak draws attention to the consequences of vaccine hesitancy and the critical importance of maintaining high vaccination coverage.
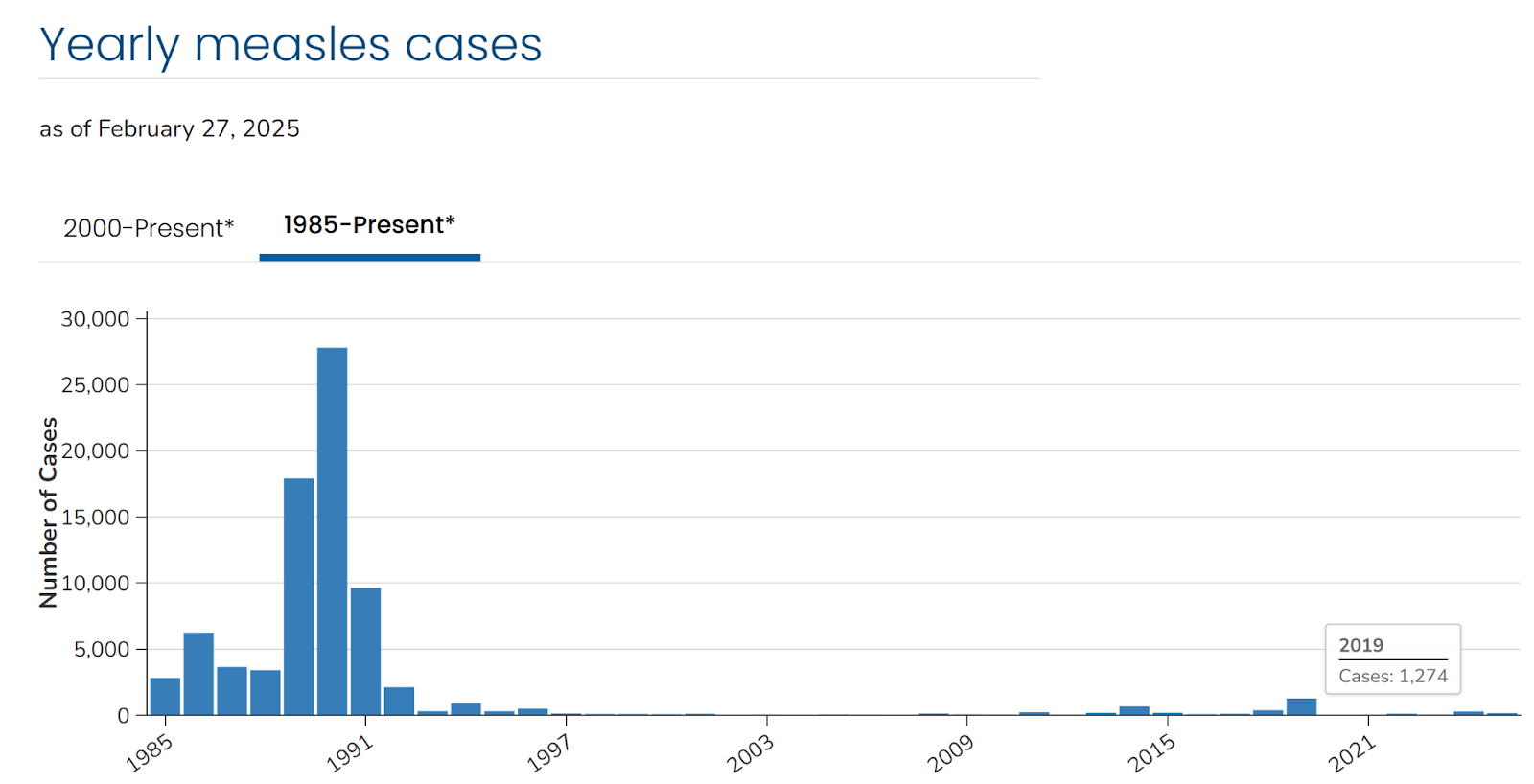
Since 2000, typically <100 cases of measles are documented in the US each year. But in 10 of those years, there were >100 cases. The highest numbers of cases were reported in:
- 2011: 220 cases
- 2014: 667 cases
- 2018: 381 cases
- 2019: 1274 cases
- 2024: 285 cases
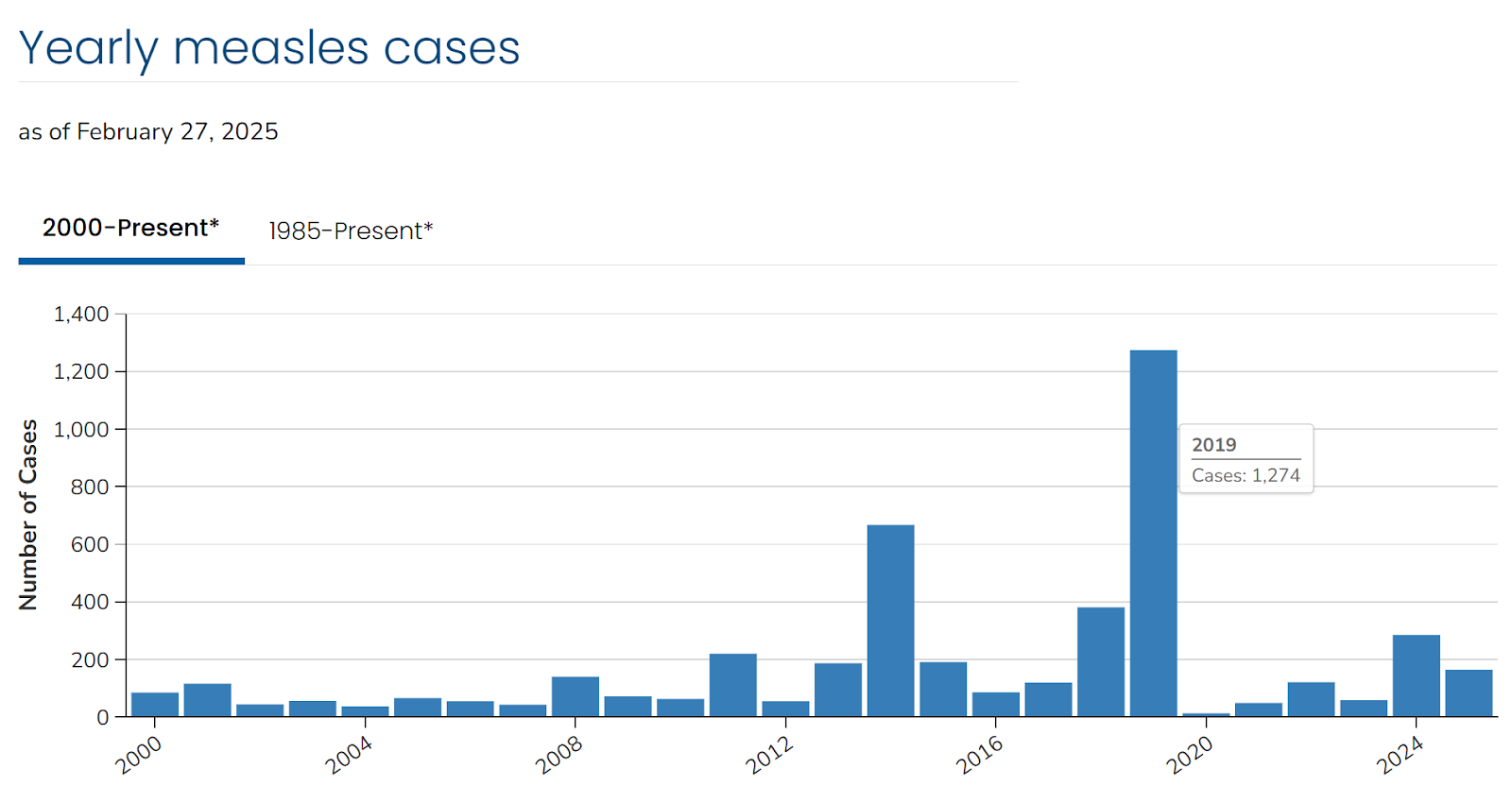
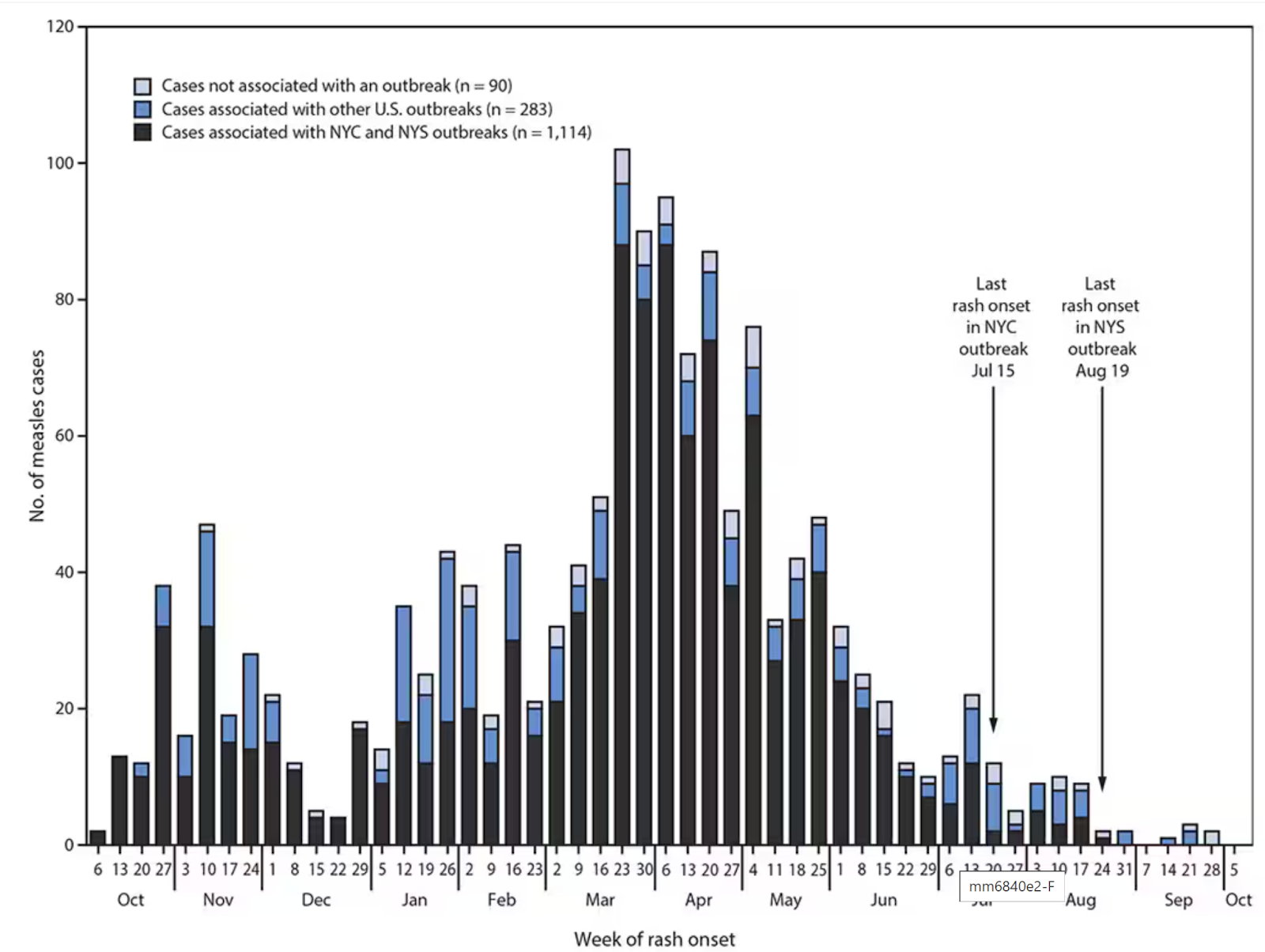
In 2025, the CDC has recorded 146 measles cases thus far, compared to 285 cases all of last year. This is trending to be the most severe measles outbreak since 2019, when the US recorded 1,249 cases between Jan to Sep 2019, the highest in 25 years and threatened our measles elimination status. It included two outbreaks in the New York Orthodox Jewish community. In total, 89% of cases were among unvaccinated individuals or those with unknown vaccination status; 10% of patients required hospitalization.
The 2019 epidemic curve showed an increase in cases during the first half of the year, followed by a gradual decline. International travelers introduced the virus in the US and it was able to spread in under-vaccinated communities, leading to multiple concurrent outbreaks.
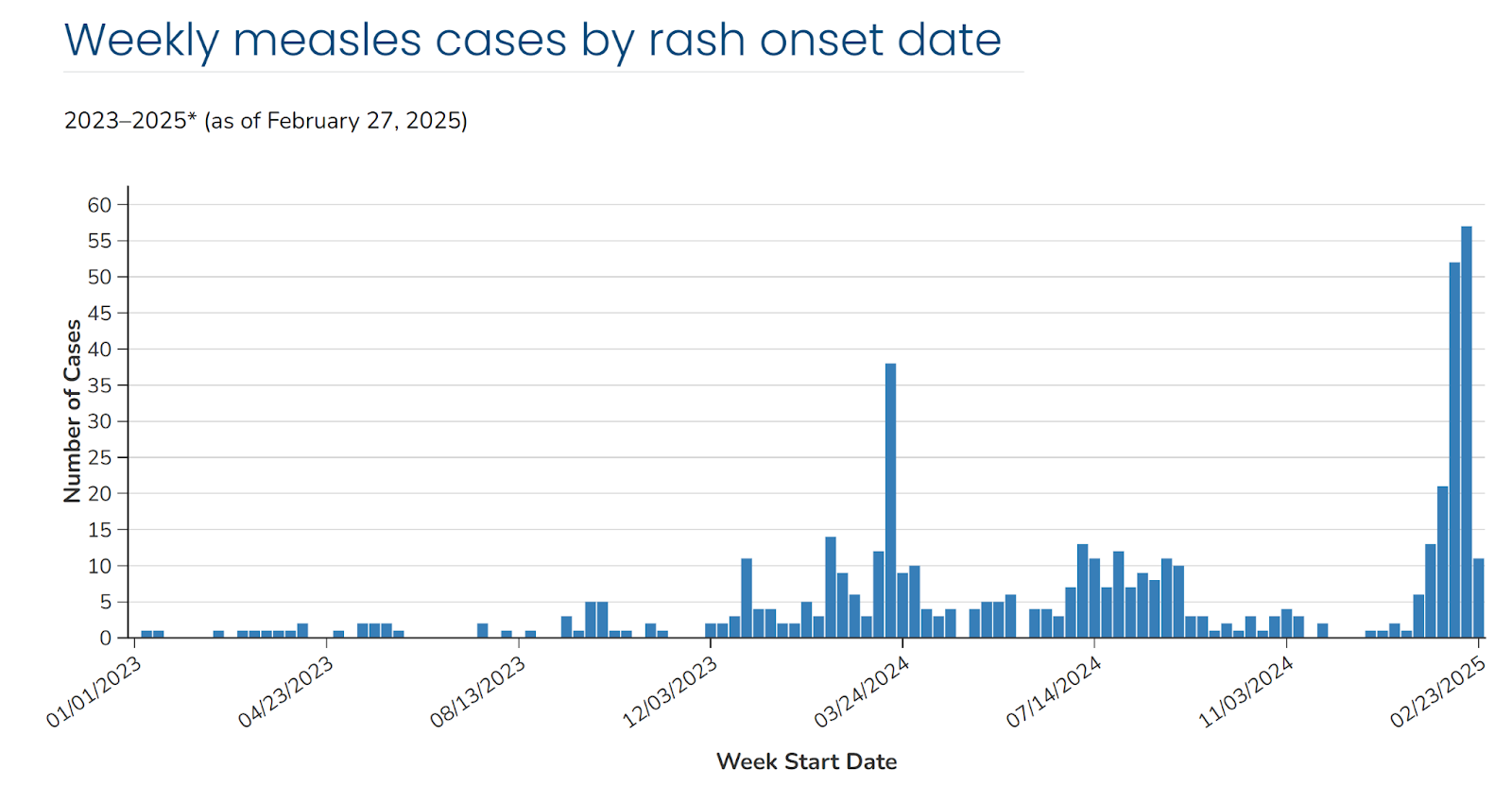
The current 2025 outbreak, while still evolving, has a lower total case count but is concentrated in specific regions, particularly Texas. While still in the early stages, the epidemic curve suggests a more localized but intense outbreak. It appears to be driven by declining vaccination rates in certain areas due to vaccine misinformation and hesitancy.
The high transmissibility of measles
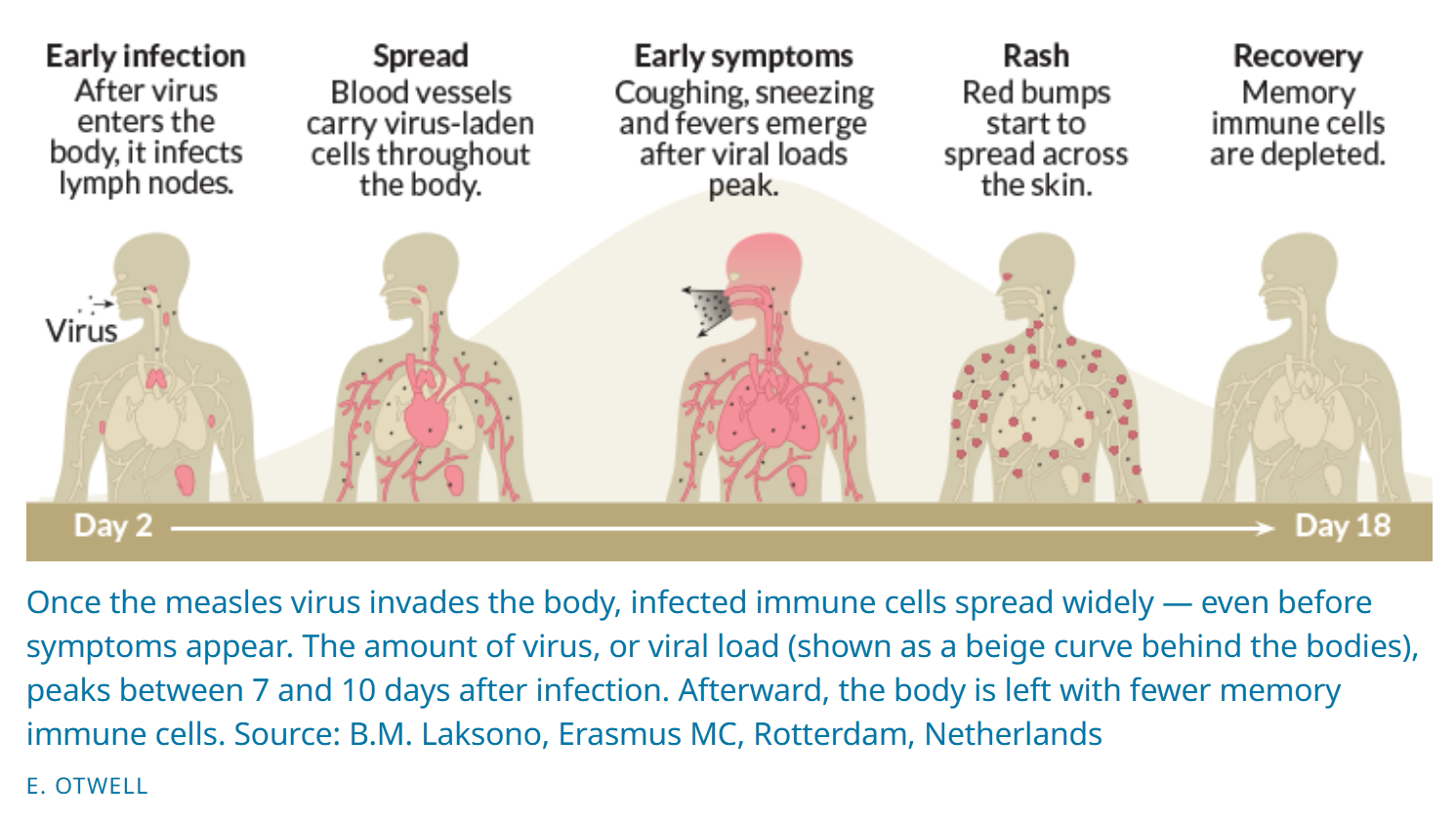
Measles is an extremely contagious viral disease that is spread via respiratory droplets. The virus can live for up to 2 hours in an airspace or on surfaces after an infected person leaves an area. Its R0 is often cited as 12-18, meaning that each person with measles would, on average, infect 12-18 other people in a totally susceptible population. That means up to 9 out of 10 people nearby an infected individual will become infected if they are not protected. An unvaccinated individual has a 90% chance of contracting measles if exposed.
Symptoms include high fever, cough, runny nose, conjunctivitis, and a distinctive red rash that often begins on the face and spreads down the body. Severe complications can occur, especially in children under 5, and include pneumonia, encephalitis (brain swelling), and death.
What you can do
On an individual level, you can protect yourself, your loved ones, and your community by ensuring you and your family are up-to-date on the MMR vaccine. The CDC recommends that children receive the first MMR dose at 12-15 months of age and a second dose at 4-6 years of age before school entry. There is also a need for adults to verify their vaccine status, especially if you are immunocompromised, a college student, traveling abroad, a healthcare professional, in close contact with immunocompromised people, or living in areas affected by the current outbreak. Adults who received an inactivated measles vaccine between 1963-1967 should be revaccinated, due to short-lived immunity. Unvaccinated individuals living or visiting affected areas should avoid public places and seek medical advice if knowingly exposed to an infected individual.
A coordinated state and federal response is necessary
To control the current measles outbreak, state and federal officials need to implement a coordinated public health strategy. This includes addressing misinformation about vaccine safety and improving vaccination rates through public awareness campaigns, as well as ensuring barrier-free and equitable access to vaccines. In Texas, health authorities are actively promoting the MMR (Measles, Mumps, and Rubella) vaccine and monitoring vaccination rates, especially in communities with low coverage.
Federal support will be essential to provide resources and guidance to affected regions. At this administration’s first cabinet meeting on February 26th, RFK Jr, our current HHS Secretary, downplayed the severity of the outbreak, inaccurately implying that hospitalizations were mainly for quarantine purposes and that such outbreaks are common. He said:
“We are following the measles epidemic every day. I think there’s 124 people who have contracted measles at this point, mainly in Gaines County, Texas. Mainly, we’re told, in the Mennonite community. There are two people who have died. We’re watching it, and there are about 20 people hospitalized, mainly for quarantine. We’re watching it, we put out a post on it yesterday, and we’re going to continue to follow it. Incidentally, there have been four measles outbreaks this year in this country. Last year, there were 16. So it’s not unusual. We have measles outbreaks every year.”
Two days later, he walked back some of that sentiment in a post on X and acknowledged the seriousness of the outbreak. He pledged the following from HHS:
- Support for Texas Department of Health through technical assistance and vaccines (including 2K MMR doses through immunization program)
- Lab support to better track the measles virus
- Daily communication with public health officials in all affected areas to support their response and ensure they have necessary resources
- Communications materials for the affected populations
- Up to date CDC website with guidance on measles management to include physician-administered outpatient vitamin A
- Continued funding for Texas’ immunization program
(We’ll dive into vitamin A further below.)
In an Op-Ed on Fox News published March 2nd, RFK Jr continued to express concerns over the outbreak. He emphasized the importance of vaccination for both individual and community protection, and outlined steps HHS is taking to support Texas health authorities. This includes “offering technical assistance, laboratory support, vaccines, and therapeutic medications as needed”. He also promised “radical transparency to regain the public’s trust in its health agencies”.

This is a notable shift from his initial misstep at the Cabinet meeting. It signals a more constructive approach to public health leadership. One that, if followed through effectively, could strengthen our response to this outbreak. While these are encouraging signs from RFK Jr, I still worry about how the mass layoffs at NIH, CDC, and other NIH agencies will impact their response capabilities.
Debunking MMR vaccine myths
RFK Jr, while staunchly arguing he is not “anti-vax”, has a history of promoting vaccine misinformation. He has falsely linked vaccines to autism, a claim thoroughly and reliably debunked.
He wrote in a forward to a 2021 book that Americans have been “misled … into believing that measles is a deadly disease and that measles vaccines are necessary, safe, and effective.” And measles outbreaks “have been fabricated to create fear” to “inflict unnecessary and risky vaccines on millions of children.”
The fact is this: the MMR vaccine is safe and effective, with no credible evidence linking it to autism or other serious health issues.
Myth: Measles is just a mild childhood illness
Truth: Before vaccines, hundreds of children died from measles annually in the US, and millions worldwide. Measles can cause pneumonia, brain swelling, and death. Even survivors can suffer "immune amnesia," weakening their protection against other diseases for years.
Myth: Better hygiene eliminated measles, not vaccines
Truth: Sanitation helps to control some diseases, but measles is so contagious that only vaccination stops it. The US had millions of measles cases per year until vaccines reduced the number of cases by 99%. Measles still spreads in high-income countries when vaccination rates fall.
Myth: The MMR vaccine causes autism
Truth: This claim originated from a fraudulent 1998 study that has been retracted and debunked. Numerous studies involving millions of children have confirmed there is no causal association between the MMR vaccine and autism.
Myth: Natural infection is better than vaccination
Truth: Measles can weaken immune memory, leaving kids more vulnerable to other infections for years following infection. The MMR vaccine provides strong, long-lasting immunity without the risk of severe illness or death.
Myth: Vaccines don’t work because some vaccinated people still get measles
Truth: No vaccine is 100% effective, but two doses of MMR protect 97% of people. Measles outbreaks happen because too many people remain unvaccinated, compromising herd immunity, not because the vaccine fails.
What about Vitamin A and Measles?
What It Does and Doesn’t Do
As signaled by RFK Jr, the CDC recently updated their recommendations to include the “administration of vitamin A under the supervision of a physician for those with mild, moderate, and severe infection”. In his Fox News Op-Ed, he cited a 2010 systematic review of clinical trials and quasi-experimental studies to suggest that “vitamin A can dramatically reduce measles mortality”. Sudfeld et al identified six high-quality RCTs and found no significant reduction in measles mortality with vitamin A treatment. But in a subgroup analysis of 3 RCTs that included multiple doses of vitamin A, receiving at least two doses of 200,000 IU for children and 100,000 IU for infants was associated with a reduction in measles mortality by 62% (95% CI 19% to 82%).
As the article indicates, the WHO does recommend vitamin A supplementation as supportive therapy to reduce severe complications for measles patients.
Measles can deplete vitamin A levels, which increases the risk of severe complications, including blindness, pneumonia, and death, especially among malnourished children.
Some studies suggest vitamin A supplementation (given to two high doses) can help to restore immune function and may be effective in reducing total mortality and complications from measles infections in younger children, particularly eye damage and blindness. But notably (and missing from RFK Jr’s and CDC’s advocacy), it is likely to be more effective in populations suffering from nutritional deficiencies.
Vitamin A does not prevent measles infection and should never be used instead of vaccination. No supplement can stimulate immunity. Only the MMR vaccine can. Vitamin A cannot “cure” measles. And there is no antiviral treatment for measles. Once infected, the virus must run its course.
Bottom Line: Vitamin A is a supportive treatment for malnourished individuals. It’s not a substitute for vaccination. And it won’t prevent the virus from spreading.
Cutting through the Noise
The current measles outbreak reminds us that scientific progress is only as strong as our commitment to maintaining it. Vaccine hesitancy and misinformation campaigns are negatively impacting our herd immunity. While challenges remain, we have the tools to prevent future outbreaks. The question is not whether we can stop measles, but whether we will.